


I will soon switch from taking 15 mg. of Xarelto twice/day to taking 20 mg. once/day. As I’ve written before, I am on blood thinner to treat the clot (deep vein thrombosis or DVT) caused by my chemo port.
Picking up the new pills kept me up that night, but only because I couldn’t get this visual pun out of my head:
As my medical oncologist has said, there’s a small chance that anastrazole may have played a role in the clot. Having quizzed others on my medical team about anastrazole, I also raised the issue with my pharmacist.
His response to my radiation oncologist’s statement that anastrazole has been shown to increase disease-free survival but not overall survival was that this is true for many drugs, like those for hypertension or cholesterol. I got the impression that this was not a bad reflection on anastrazole, but instead was a fairly standard limitation among medications in general. Good to know.
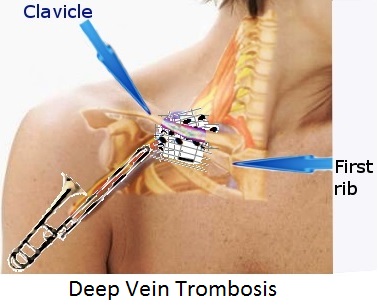
The medical image used above is from Medscape’s info on subclavian vein thrombosis, which states, “The incidence of this condition has increased remarkably over the past two decades because of the extensive use of central venous catheters in patients with cancer and other chronic medical conditions. The demand for a more standardized treatment of subclavian vein thrombosis is growing. However, until randomized data from well-designed trials are available, absolute statements about treatments cannot be made.”
The more I read, the more it strikes me that (1) my type of port-induced blood clot is viewed as rare, but (2) the frequency of subclavian DVT is growing over time. In other words, subclavian DVT is rare because the technology is still relatively young. According to Nursing Link, “The use of implantable ports has grown tremendously since their first use in 1981….with more than 100,000 ports being implanted each year.”
A small study published in 2010, covering the period from July 2007 to July 2008, found that, among 92 patients with ports, initial ultrasound showed that 64 had developed thrombi around the catheter without obstruction of venous flow and 3 had developed thrombi with obstruction of venous flow. Within a month, 4 patients with thrombi but no obstruction had developed an obstruction. Three others had developed an obstruction after one month. Of those, one patient had developed a pulmonary embolism.
My surgeon had told me that subclavian DVTs occur in about 3 percent of cases. Ports have been in use for 35 years. To keep the math simple, 35 years x (at least) 100,000 ports implanted per year = 3,500,000 implanted ports. Three percent of that = 105,000 patients who develop DVTs, or an average of 3,000 patients per year.
However, if we use the results of the study performed in 2007-2008 – with the caveat that this is not a robust test due to its small numbers – the percentage of patients developing DVT with obstruction rises to 7 out of 92, or 7.6 percent. If we apply that percentage to the whole, the patients who develop DVTs with obstruction = 7.6 percent of 3,500,000 implanted ports, which is 266,000, or an average of 7,600 patients per year. (I am treating 100,000 patients getting ports per year as an average over 35 years, rather than as the result of an increase in implantations over time, because I don’t have a longitudinal frequency curve.)
The bottom line is that the port-DVT relationship needs more study. The technology is sufficiently new that we just don’t have enough data to reach a strong conclusion. Port-associated DVTs may be rare because they really are rare (relatively speaking), or because the truly accurate numbers haven’t been generated yet and it’s too soon to really know.
Having said all that, I would get a port again if the occasion arose (which I hope it never does). Given my situation, the benefits still outweigh the risks.

I did this up for Valentine’s Day, using stencils made from images in Beeton’s Book of Needlework.
Here I embellished an altered photographic self-portrait from about two years ago with a stencil made from William Peck’s The Constellations and How to Find Them.
Lately I’ve been listening while doing my workouts to Vol. 2 of Edward Gibbon’s The History of the Decline and Fall of the Roman Empire, a free audiobook courtesy of LibriVox. I hadn’t exercised while listening to an audiobook before and have been enjoying the experience. I had read the ebook of Volume 1, courtesy of Project Gutenberg.
I am also about 4/5 through the extraordinary The Death of Cancer, written by Vincent T. DeVita Jr., MD and Elizabeth DeVita-Raeburn. I had learned about this book through Malcolm Gladwell’s New Yorker article “Tough Medicine”.
Gladwell writes, “DeVita’s book is nothing like Siddhartha Mukherjee’s magisterial ‘The Emperor of All Maladies.’ Mukherjee wrote a social and scientific biography of the disease. DeVita, as befits someone who spent a career at the helm of various medical bureaucracies, has written an institutional history of the war on cancer. His interest is in how the various factions and constituencies involved in that effort work together – and his conclusions are deeply unsettling.”
I’ll say. This book gets into the nitty gritty, medical and political sausage making behind cancer treatment and research. Highly recommended.
Loading comments...