


Disclaimer: I wrote most of this entry before I spoke with Dr. W on April 16, 2015. I have left it as-is because I wanted to show my raw reaction to what I had seen. The Update section reports on our conversation.
Currently making the rounds is the finding that among women ages 40-59, overdiagnosis of breast cancer from screening mammograms costs $4 billion annually – much higher than previously documented. This discovery further fuels the debate over the value of mammograms.
Given my recent discovery about my own mammograms, I find this story ironic. Here’s why:

To my layman’s eye, my tumor stands out like a sore thumb. Also to my layman’s eye, the tumor in my screening mammogram from 2013 and that from last year look virtually identical. I was still in the process of reaching my goal weight, so I was 23 pounds heavier on the day of my 2013 mammogram than I had been on the day of last year’s mammo. I had informed the technician of this, because weight changes affect fat deposition in the breast, which can in turn affect the images.
Other than that, what is the difference between these two tumor images?
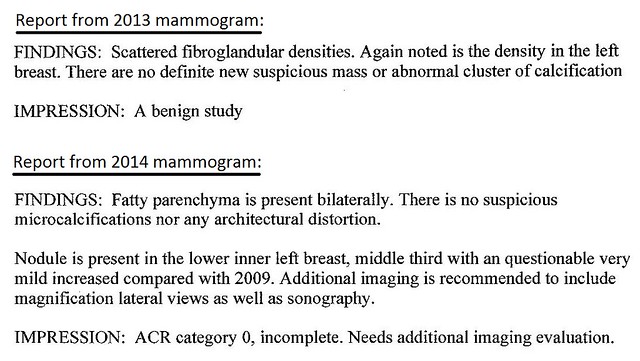
Both mammograms had been taken at the same facility and on the same machine. The difference: my 2013 tumor, now known to have been cancerous, had been labeled “benign.” My 2014 tumor had been viewed as suspicious.
Another difference: The images in 2013 had been reviewed by Dr. K, while those in 2014 had been reviewed by Dr. W.
Two different doctors. Two different pairs of eyes. Two different conclusions.
To say I am lucky is a vast understatement; I feel as though I’ve dodged a real bullet here. I’ve been saying that my screening mammogram in 2014 had saved my life. I now tweak that statement: my screening mammogram and Dr. W had saved my life. Dr. W had been the one who had pulled the alarm. Otherwise, I wouldn’t have known a thing. (Several months ago, Dr. W – who had also performed my biopsy – had given a talk on breast imaging at my local breast cancer support group.)
I am also very, very lucky in that my tumor had been an invasive colloid (mucinous) carcinoma, which is relatively non-aggressive. So non-aggressive that it had experienced a “questionable very mild increase” from 2009 to 2014. That’s five years – at least – that I had been walking around with that cancer inside me. (In 2009 I was still pre-menopausal. Had my cancer been discovered then, I likely would have been placed on tamoxifen rather than anastrazole. What else would it have meant in terms of my treatment?)
I did not see the image from my 2013 mammogram until April 10, 2015. I probably wouldn’t have seen it at all if my hospital had not been acquired, which requires me to change diagnostic imaging facilities. I wanted to get what records I could, to make sure that they would reach the new facility.
Images older than 2013 are “on film,” which means that I can’t have them. At best, I can pick them up from the hospital, deliver them to the new facility at the time of my next mammogram, and then return them to the hospital. The earliest I can have my next mammo is in June, six months after my completion of radiation last December.
When I have my appointment and I pick up the films to take to the new facility, you’d better believe I’m going to take a hard look at those images.
With all the focus in the news on false positives from mammograms, I want to know about false negatives. False negatives are generally associated with dense breast tissue, but that had not been the case with me. (Finding a tumor in a dense breast is like finding a polar bear in a blizzard; there’s just too much noise. This post by James Marroquin includes a comparison shot of what a tumor looks like in a dense versus a non-dense breast.)
According to the National Cancer Institute (NCI), “Overall, screening mammograms miss about 20 percent of breast cancers that are present at the time of screening.” Most false negatives occur as a result of dense breasts, but I want to know what percentage occurs the way that mine had, not for a single screening but for at least five years. (And is that percentage calculated per year or per patient?) For those five years I had received my usual statement from the hospital saying that my mammogram had been normal, when all that time I had been walking around not just with cancer, but with cancer that had been visible.
The news stories about false positives give the impression that a flock of medical Chicken Littles squawk that the sky is falling to the tune of $4 billion wasted and the traumas of unnecessary biopsies and more. I am a still-living example of the other side of that coin, one in which at least one doctor did not speak up when he should have. Because the sky was falling. It was falling for at least five years, while I believed that I walked in safety on a bright, sunny day.
To put this in perspective, I believe (but do not know for certain) that my false negatives made little difference in my overall treatment (other than tamoxifen versus anastrazole), given my tumor’s “questionable very mild increase.” That will be one of my questions to my medical team. This is all chemo under the bridge as far as I’m concerned, but I still have a right to know.
But what about people whose tumors are more aggressive than mine had been? How many receive reports of a “normal mammogram” when in fact a tumor exists and stands out as mine had? Without Dr. W, how much longer might I have gone with year after year of “normal” reports? What are the chances that my tumor would have progressed beyond Stage Ia, because a doctor saw no need for further investigation of a visible mass?
I want to ask Dr. K (who now works in a different state) how he had decided that my cancerous tumor had been benign. Was it part of his training? Was he afraid of potentially contributing to that $4 billion worth of “unnecessary” follow-ups? Was there any pressure put on him to not push for clarification?
Diagnostic imaging is fraught with uncertainties. After Dr. W had pulled the alarm on my screening mammogram last year, my diagnostic mammogram and ultrasound had been reviewed by Dr. Z. Dr. Z told me that of the images he has seen that are like mine, half were cancerous and half were benign. Faced with that uncertainty, he had recommended a biopsy. Thank goodness he had.

My take-away: Get your images. I now ask my imaging facility for a CD, which I receive along with written records. It’s my body; it’s my data. I know full well that as a layperson I am not trained to differentiate a benign calcification from a malignant tumor; but as my case has shown, doctors trained in this area also make mistakes. Dr. W saw what Dr. K did not.
A “normal mammogram” letter does not necessarily mean that nothing is there.
A biopsy – and those billions of dollars’ worth of “extra” procedures – may not always be needed, but at the very least it pays to have an extra pair of eyes.
Update: I stopped at the hospital on April 16, to at the very least drop off a thank-you card and letter for Dr. W. Fortunately, she was available for me to speak with her. I had my mammogram CDs and printouts with me.
She spent good, quality time with me and we reviewed the images from 2013 and 2014 (earlier images were not accessible in her office). I learned the following:
-
Dr. K had functioned within the “standard of care.” If anything, Dr. W had exceeded that standard because my 2014 images had bothered her sufficiently for her to flag them. Dr. K’s error had been exactly that, within a field that remains imprecise.
-
An irregularity such as mine that remains unchanged for three years is considered to be benign (even if it ends up being malignant). Viewed from one angle, my 2013 nodule image appeared to have a smooth edge (benign). Viewed from another angle, it had angularity (suspicious). Again, my cancer had been very slow-growing.
-
Dr. W did not know the proportion of false negatives like mine as compared with the much more prevalent false negatives that occur with dense breasts. She said she didn’t know if any such study had ever been done, and said that the proportion of false negatives like mine is probably very small.
-
With respect to the debate over the value of mammograms, she said, “Don’t get me started.” (She is a strong proponent of mammograms.)
I told her I wanted to write to Dr. K, to provide feedback and to inform him of his error. Now that I know that his mistake had occurred within acceptable parameters, I wanted to make sure that the tone of my letter was non-threatening. I’m thinking of people whose cancer might be more aggressive, for whom such an error could have greater consequences. According to NCI, a mammogram can be graded as “probably benign,” with a follow-up mammogram recommended for six months rather than a year (as a grade of “benign” would indicate).
All things considered, my talk with Dr. W gave me peace of mind. It still bothers me that my malignant tumor had been labeled benign for years, but my case is an outlier and a non-aggressive one at that.
That said, I still want to get my mammogram images and reports as we go forward.
Addendum: Rebecca Hogue is conducting a study on the impact of cancer blogs. If interested, you can access her survey here.
Loading comments...